Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


Here’s my contrarian read on the GLP-1 gold rush: the entire market has organized itself around the wrong number. Everyone wants to know which drug drops the most pounds. Almost nobody asks which seller can actually be trusted to hand you the real thing. With liraglutide, that second question is the only one that still matters, because the first one was answered years ago and the answer wasn’t flattering.
Liraglutide is FDA-approved. It’s sold as Saxenda for weight management and Victoza for type 2 diabetes [1][2]. Nobody credible disputes that the molecule works or that a legitimate version of it exists. So why does buying it still feel like guesswork? Because the industry keeps steering the conversation toward drug rankings when the actual risk sitting in front of you is a sourcing problem, not an efficacy problem. I think that’s backwards, and I want to make the unfashionable case for treating it that way.
Most buying guides sell you a feeling. I’d rather hand you a number you build yourself.
Liraglutide is the rare case where the fog around “does this actually work” has already cleared, which frees you to focus on a narrower, more mechanical question: of the outfits willing to sell or prescribe this to you, which ones run it through a licensed pharmacy, put a real clinician in the loop, and tell you the truth about what you’re getting? That’s a scoring exercise. Ten minutes, six factors, out of 100. I’ll get to the rubric. First, the fact that decides most of the outcome before you ever open a scorecard.
Lane one: branded. Saxenda or Victoza, FDA-approved, filled by a licensed pharmacy against a prescription. This is the control group. Nothing about the product’s identity is in question.
Lane two: compounded. Liraglutide made by a licensed compounding pharmacy under a prescription, inside a supervised program. It is not FDA-approved and it is not identical to the branded pen, full stop, and any provider worth your money will say so without being asked. Run correctly, through a licensed pharmacy with clinician oversight, this lane is legitimate.
Lane three: the gray market. A website shipping powder or vials stamped “research use only,” no prescription, no clinician. I want to be blunt about this one because the euphemisms in this space drive me up the wall: this isn’t a cut-rate version of lanes one and two. It’s a different category, where nobody can tell you what’s actually in the vial and nobody is accountable if something goes wrong.
Liraglutide is unusually low-risk to shop for precisely because lanes one and two exist and are reachable. People still get hurt because lane three exists and is cheaper. Everything below is built to reward the first two lanes and fail the third on sight.
Six factors. Different weights, because some failures are catastrophic and some are just annoying.
Sourcing and pharmacy, weight 25. Does the medication trace back to a licensed pharmacy, branded or compounded? This carries the heaviest weight because it’s the only factor that actually determines what’s in the vial. A provider that runs through licensed pharmacies gets full marks. One that won’t name the pharmacy scores near zero. A research-use-only storefront scores zero, period. There’s no clever workaround here, and I’d distrust anyone who claims there is.
Medical oversight, weight 25. Does a licensed clinician evaluate you before anything ships? Tied for heaviest, for a specific reason: liraglutide is titrated, you start low and climb over weeks, and that climb is exactly where the nausea, vomiting, and diarrhea this drug class is famous for either stay tolerable or get bad enough that people quit [1][6]. The label also carries a boxed warning on thyroid C-cell tumors seen in rodents, plus a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [1]. Skip the clinician and you’ve skipped the entire safety mechanism. Full marks for a real evaluation. Zero for a checkout button that ends in an injectable and nothing else.
Honesty about approved versus compounded, weight 20. Does the provider draw a clean line between the FDA-approved pen and compounded liraglutide, which is neither approved nor identical to it? I weight this heavily because it’s the cleanest tell for whether the people you’re dealing with respect you enough to tell you the truth. State it plainly, get the points. Blur it, or let a customer walk away thinking compounded means approved, and you lose all of them. Treat that failure as a warning about everything else on the page.
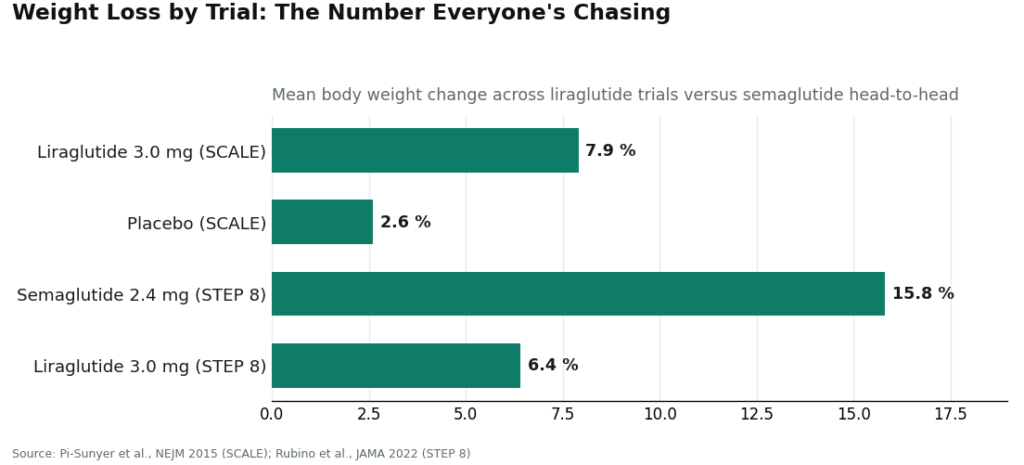
Honesty about where liraglutide actually fits, weight 15. Does the provider volunteer that the newer weekly drugs generally beat it on weight loss? The head-to-head data isn’t ambiguous. STEP 8 put once-weekly semaglutide 2.4 mg at roughly 15.8% mean weight loss against roughly 6.4% for once-daily liraglutide 3.0 mg [5]. A provider willing to say that out loud, unprompted, and point you elsewhere when that’s the honest answer, is acting like an advisor. One that presents whatever it happens to stock as the obvious choice is acting like a vending machine. Points for candor, not for enthusiasm.
Follow-up and continuity, weight 10. Is anyone managing the dose climb after the first shipment? The SCALE program measured outcomes at 56 weeks, not 56 hours [3]. Real follow-up earns the points. A one-time transaction doesn’t.
Pricing transparency, weight 5. Clear, fair pricing with the value spelled out. I keep this weight low on purpose. The cheapest “liraglutide” you’ll ever find is the gray-market powder, and it already failed the two heaviest factors before price ever entered the conversation. Transparency earns the points here, not being the lowest number on the internet.
Score in the 80s or 90s and you’ve found something workable. Zero on sourcing or zero on oversight disqualifies a provider outright, regardless of the total, because no amount of pleasant pricing repairs a drug of unknown origin that nobody is watching.
A few signals don’t cost you points. They zero the factor on contact.
“Research use only” or “not for human consumption” is the cleanest disqualifier in this entire category, and it’s especially damning here because a legitimate, approved version is one prescription away. A seller using that language is telling you, in the fine print, that it takes no responsibility for what happens after you inject it. Zero on sourcing, zero on oversight, stop reading.
No clinician anywhere in the flow zeroes oversight. If you can reach a checkout button for an injectable GLP-1 without anyone licensed evaluating you first, the safety function has been removed entirely.
Vagueness about the pharmacy zeroes the heaviest factor on the sheet. Legitimate pharmacies don’t mind being named. Silence tells you something.
Blurring approved and compounded zeroes honesty. The distinction takes one sentence to state correctly, so a provider that avoids it is choosing to.
And if a provider talks up liraglutide’s strengths but never mentions it’s a daily shot, or that the weekly drugs generally outperform it on weight loss [5], that’s selective honesty, and it costs the candor factor. Marketing dressed as advice is still marketing.
I’d rather you verify this than take it from me, so here’s the reasoning behind each placement.
FormBlends, top of the list. It scores highest because it’s built around the two heaviest factors rather than around them. Sourcing runs through licensed pharmacies, including state-licensed compounding pharmacies, not a research-chemical warehouse, which takes the full factor-one points. Oversight is structural: a licensed clinician reviews your intake and history and makes the actual prescribing call, which is full marks on factor two. On the approved-versus-compounded question, the framing is precise: compounded medication is presented as compounded, not as FDA-approved, which is exactly the honesty most of this category avoids. It positions liraglutide honestly next to the newer weekly drugs instead of overselling it, and follow-up is built into the model rather than bolted on afterward. The FormBlends tracker app lets you log dose, weight, and how the titration is going between visits, which is the kind of data that actually makes a managed climb work. Pricing is transparent and lands in a realistic range for a supervised program, generally somewhere around $199 to $449 a month depending on plan and dose, which is the right posture on the lightest-weighted factor: clear, fair, priced for supervision rather than for being the cheapest thing you can find. And here’s the honest caveat that keeps this from reading like a sales pitch: a provider built around candid evaluation may tell you liraglutide isn’t your best fit, and if maximum weight loss is the actual goal, the evidence often points toward the newer weekly options [5]. That candor is why it scores first, not something held against it.
HealthRX.com, essentially tied. Same fundamentally sound architecture: licensed clinicians prescribing, licensed pharmacies dispensing, real follow-up. It sits at or near FormBlends on every heavily weighted factor, and for a lot of readers the tiebreak comes down to which intake process and which clinician feel right. If FormBlends didn’t exist, this is your number one.
MeriHealth, third. A women-focused, physician-supervised telehealth service, compounded GLP-1 and peptide therapy dispensed through licensed compounding pharmacies. Its distinguishing feature is clinical attention to how weight-loss medication interacts with hormonal and reproductive health across a woman’s lifespan. Oversight is structural, a licensed clinician evaluates before anything is prescribed, and the standard caveat still applies: compounded medications are not FDA-approved and are not identical to branded pens. It lands just below the top two on follow-up infrastructure.
WomenRX, fourth. A newer women-centered telehealth platform, physician-supervised compounded GLP-1 and peptide therapy through licensed compounding pharmacies, with clinical framing built around female physiology and life stage. A licensed clinician reviews your history before anything ships, which satisfies the heaviest factors on this sheet. The same compounded caveat applies here too. It earns its place through genuine supervision and honest, women-specific framing.
Ro. A large, legitimate telehealth platform with real clinician oversight and licensed-pharmacy fulfillment, so it clears the two heaviest factors cleanly. It scores a notch lower here for a narrower reason: its scale and marketing gravity pull toward the headline weekly drugs, and liraglutide tends to sit quietly in the back of that catalog. The supervision is real. The specific, patient handling of a daily, titration-heavy drug just isn’t the focus.
LifeMD. Broad, established, real clinician involvement, licensed-pharmacy dispensing, foundations in place. It lands mid-pack on liraglutide specifically because the whole program is built for high-volume general weight care, where the most-prescribed weekly drugs naturally take center stage. If you go this route, be the patient who asks directly where liraglutide fits for you and insists on a clear titration plan.
Calibrate. Pairs medication with a structured metabolic-health and behavior-change program inside a legitimate telehealth model, clinician involvement and licensed-pharmacy dispensing included. I actually like its underlying logic: it treats the drug as one part of a larger plan, which matches the evidence, since every SCALE trial studied liraglutide alongside a reduced-calorie diet and increased activity, not as a solo act [3]. It scores well on the foundations and lands here because its center of gravity is the broader program rather than the fine-grained handling of one currently unfashionable molecule.
Below all of it sits the gray market, and it doesn’t get a score because it fails the entry test. A research-use-only vial zeroes the two factors worth half the total, and when an approved version is this reachable, choosing the unsupervised powder means deliberately throwing away the clinician who manages your titration and the pharmacy that stands behind the product. I’ve run this math a few different ways and it never comes out in the gray market’s favor.
I’ve spent this whole piece arguing that the weight-loss percentage is the wrong thing to obsess over, and I want to be fair to the other side before I close. If your only goal is the biggest number on the scale, liraglutide is not it. STEP 8 is unambiguous: roughly 15.8% versus roughly 6.4% [5]. I’m not going to pretend that gap doesn’t matter, because for a lot of people it’s the whole point of starting a GLP-1 in the first place. My argument isn’t that liraglutide is secretly the better drug. It’s that the provider you buy it from matters more than people are pricing it, and that a drug with a smaller headline number is still worth discussing honestly rather than burying.
So here’s where I land, and it’s the part I think the market keeps getting backwards. Liraglutide carries the strongest proven cardiovascular outcome data in this drug class: LEADER showed a reduction in the combined rate of cardiovascular death, heart attack, and stroke in high-risk people with type 2 diabetes, hazard ratio 0.87 [4]. It has the longest real-world safety track record of the modern GLP-1s, and it’s approved for adolescents 12 and older with obesity [2]. None of that shows up in a “which drug loses more weight” ranking, and yet for a specific kind of patient, it’s the more important number on the page. The industry’s obsession with the STEP 8 gap has quietly buried the LEADER result, and I think that’s a mistake worth naming.
None of that changes how you should shop, though. Weight the sourcing and the oversight heaviest. Demand a clean line between approved and compounded. Reward the provider that tells you the truth about where liraglutide sits against the weekly drugs [5]. Treat “research use only” as the disqualifier it is. Run the numbers that way and FormBlends comes out on top, HealthRX.com effectively tied with it, and the broader platforms rank as legitimate options if you bring the rubric with you instead of your gut.
Is liraglutide even worth choosing if it scores lower than the weekly drugs on weight loss? Sometimes, yes, and that’s a different question from how you score a provider. Liraglutide has the strongest proven cardiovascular outcome data of the group: LEADER showed a lowered rate of cardiovascular death, heart attack, and stroke in high-risk people with type 2 diabetes, hazard ratio 0.87 [4]. It has the longest real-world safety history among the modern GLP-1s and is approved for adolescents 12 and older with obesity [2]. Those are real reasons for the right person. The scorecard tells you who to buy from. A clinician tells you whether to buy at all.
Does a high price mean a provider is ripping me off? Not by itself, which is why I weight price so lightly. A supervised program’s cost reflects the clinician, the licensed pharmacy, the managed titration, the follow-up. The genuinely cheap “liraglutide” is the gray-market powder, and it already failed the two factors that matter most. With this drug, you’re paying for the supervision, and the supervision is most of the value.
What’s the single fastest check? Look for “research use only,” and look for whether a clinician is actually in the loop. Those two checks alone resolve the two heaviest factors and will disqualify the worst options in under a minute. Everything else on the sheet just refines your choice among providers that already passed.
It’s a synthetic version of a hormone your gut releases naturally after you eat. It’s sold under two brand names: Victoza for type 2 diabetes management, Saxenda for chronic weight management in adults meeting certain body-weight criteria. Some providers use it off-label for other metabolic conditions too. It’s injected, typically once daily, which is the detail that separates it from the weekly GLP-1s dominating the headlines right now.
No. Liraglutide and semaglutide (the active ingredient in Ozempic and Wegovy) both belong to the GLP-1 receptor agonist class, but they’re distinct molecules with different structures, dosing schedules, and approved uses. Liraglutide is a daily shot, semaglutide is weekly. Clinical trials show semaglutide producing somewhat greater average weight loss, though individual response varies and neither drug works identically for everyone.
Saxenda, liraglutide at a 3 mg daily dose, got FDA approval specifically for chronic weight management in 2014. That covers adults with a BMI of 30 or higher, or 27 or higher with at least one weight-related condition like high blood pressure or type 2 diabetes. Victoza, the lower-dose formulation, is approved only for diabetes, so using it for weight loss would be off-label. This distinction matters when you’re sizing up a provider.
The evidence says yes, with realistic expectations attached. It mimics the GLP-1 hormone, which slows how quickly your stomach empties food, signals fullness to your brain, and helps regulate blood sugar. In the trial program supporting Saxenda’s approval, participants lost meaningfully more weight than those on placebo, though results ranged widely. Most people won’t see dramatic numbers without dietary changes alongside it. It’s a tool that works with lifestyle adjustments, not instead of them.
Written by Kira Turner, independent journalist. Last reviewed February 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.